Pernah tak korang alami sindrom ni...rasanya ramai yang selalu menaip tak kiralah guna mesin taip ke, komputer ke atau pun gila ber 'sms', mesti akan kadang-kala rasa kebas atau sesemut dibahagian hujung jari. So kalau korang pernah apatah lagi selalu mengalami sindrom tu...eloklah korang baca artikel yang aku C&P dari wikipedia ni. Cuma pandai-pandailah korang translatekan ya...lagipun cik google pun sudi nak tolong translatekan utk korang...
Carpal tunnel syndrome (CTS), or median neuropathy at the wrist, is a medical condition in which the median nerve is compressed at the wrist, leading to paresthesias, numbness and muscle weakness in the hand. Night symptoms and waking at night is a characteristic of established carpal tunnel syndrome. They can be managed effectively with night-time wrist splinting in most patients.
The definitive treatment for carpal tunnel syndrome is carpal tunnel release surgery. This is effective at relieving symptoms and preventing further nerve damage, but established nerve dysfunction in the form of static (constant) numbness, atrophy, or weakness are usually permanent.
Most cases of CTS are idiopathic (without a specific cause). Some patients are genetically predisposed to develop the condition.
The diagnosis of CTS is often misapplied to patients who have activity-related arm pain, such as RSI.
Carpal Tunnel Syndrome History
Although the condition was first noted in medical literature in the early 20th century, the first use of the term “carpal tunnel syndrome” was in 1939. The pathology was identified by physician Dr. George S. Phalen of the Cleveland Clinic after working with a group of patients in the 1950s and 1960s.
Compression of the median nerve as it runs deep to the transverse carpal ligament (TCL) causes wasting of the thenar eminence, weakness of the flexor pollicis brevis, opponens pollicis, abductor pollicis brevis, as well as sensory loss in the distribution of the median nerve distal to the transverse carpal ligament. There is a superficial sensory branch of the median nerve, which branches proximal to the TCL and travels superficial to it. This branch is therefore spared, and it innervates the palm towards the thumb.
Work related
The international debate regarding the relationship between CTS and repetitive motion in work is ongoing. The Occupational Safety and Health Administration (OSHA) has adopted rules and regulations regarding cumulative trauma disorders. Occupational risk factors of repetitive tasks, force, posture, and vibration have been cited. However, the American Society for Surgery of the Hand (ASSH) has issued a statement that the current literature does not support a causal relationship between specific work activities and the development of diseases such as CTS.
The relationship between work and CTS is controversial; in many locations workers diagnosed with carpal tunnel syndrome are entitled to time off and compensation. Carpal tunnel syndrome results in billions of dollars of workers compensation claims every year.
Some speculate that carpal tunnel syndrome is provoked by repetitive grasping and manipulating activities and that the exposure can be cumulative. It has also been stated that symptoms are commonly exacerbated by forceful and repetitive use of the hand and wrists in industrial occupations, but it is unclear if this refers to pain (which may not be due to carpal tunnel syndrome) or the more typical numbness symptoms.
A review of available scientific data by the National Institute for Occupational Safety and Health (NIOSH) indicated that job tasks that involve highly repetitive manual acts or specific wrist postures were associated with incidents of CTS, but causation was not established, and the distinction from work related arm pains that are not carpal tunnel syndrome was not clear. It has been proposed that repetitive use of the arm can affect the biomechanics of the upper limb or cause damage to tissues. It has also been proposed that postural and spinal assessment along with ergonomic assessments should be included in the overall determination of the condition. While addressing these factors has been found to improve comfort in some studies, there is no evidence that they affect the natural history of carpal tunnel syndrome.
Psychosocial factors
Studies have related activity-related upper extremity pain with psychological and social factors, but most such pains are nonspecific but commonly mislabeled as carpal tunnel syndrome. Psychological distress correlates with increased pain at work, as do other psychosocial stressors such as job demands, poor support from colleagues, and work dissatisfaction.
As mentioned elsewhere on this page, carpal tunnel is characterized by numbness, not pain. Therefore, any associations between stress and carpal tunnel syndrome are debatable.
Examples include:
Clinical assessment by history taking and physical examination can support a diagnosis of CTS.
The role of MRI or ultrasound imaging in the diagnosis of carpal tunnel syndrome is unclear.
Recommendations for preventing carpal tunnel syndrome have poor scientific support. Current recommendations generally don't suggest immobilizing braces, but instead activity modification and non-steroidal anti-inflammatory drugs as initial therapy, followed by more aggressive options or specialist referral if symptoms do not improve.
Many health professionals suggest that, for best results, one should wear braces at night and, if possible, during the activity primarily causing stress on the wrists.
Physiotherapy
There is little evidence to support the use of physiotherapy or occupational therapy techniques for carpal tunnel syndrome. They seem to be oriented primarily towards non-specific activity related pain rather than the numbness of carpal tunnel syndrome. The following comments regarding physical therapy seem to apply more to such chronic activity related pains than to verifiable idiopathic median nerve compression at the carpal tunnel.
Physiotherapy offers several ways to treat and control carpal tunnel syndrome. This procedure should be directed specifically towards the pattern of pain / symptoms and dysfunction assessed by the therapist. As such, it may include a range of modalities ranging from soft tissue massage, conservative stretches and exercises and techniques to directly mobilize the nerve tissue. It can also include the aforementioned immobilizing braces.
Clinically, sometimes a patient will present with a hand that is very inflamed and swollen with severe symptoms of pain, tingling and numbness and almost a fear of use because of the pain. In these cases a physiotherapist may focus on techniques to reduce the pain and inflammation, and exercises to encourage improved circulation. A comprehensive review of effectiveness of hand therapies in carpal tunnel management demonstrates that there is some valid scientific evidence for a range of therapeutic modalities.
For instance, Body Awareness Therapy such as the Feldenkrais method has positive effects in relation to fibromyalgia and chronic pain. Structured exercise programs using these therapies to reduce wrist pain have been developed.
Occupational therapy offers ergonomic suggestions to prevent worsening of the symptoms and occupational therapist facilitates hand functions through functional activities and helps to regain the functions which are necessary for the functional living through remedial adaptive approaches.
Any forceful and repetitive use of the hands and wrists can cause upper extremity pain. More frequent rest can be useful if it can be orchestrated into one's schedule. It has been shown that taking multiple mini breaks during the stressful activity is more effective than taking occasional long breaks. There are computer applications that aid users in taking breaks. All of these applications have recommended defaults, following the most effective average break configuration, which is a 30 sec. pause every 3 to 5 minutes (the more severe the pain, the more often one should take this break). There are also programs that automatically click the mouse. Before investing in these types of programs, it's best to consult with a doctor and research whether computer use is causing or contributing to the symptoms, as well as getting a formal diagnosis.
More pro-active ways to reducing the stress on the wrists which will alleviate wrist pain and strain involve adopting a more ergonomic work and life environment. Switching from a QWERTY computer keyboard layout to a more optimised ergonomic layout such as Dvorak was commonly cited as beneficial in early CTS studies, however some meta-analyses of these studies claim that the evidence that they present is limited.
It is also important that one's body be aligned properly with the keyboard. This is most easily accomplished by bending ones elbows to a 90 degree angle and making sure the keyboard is at the same height as the elbows. Also it is important not to put physical stress on the wrists by hanging the wrist on the edge of a desk, or exposing the wrists to strong vibrations (e.g. manual lawn mowing). Position the computer monitor directly in front of your seat, so the neck is not twisted to either side when viewing the screen.
Exercises that relax and strengthen the muscles of the upper back can reduce the risk of a ''double crush'' of the median nerve.
Massage is one of the most overlooked methods for treatment of the symptoms of CTS. The use of myofascial release and active stretch release can erase the pain, numbness, tingling and burning in minutes. Then following up with the stretches and exercises afore mentioned will lengthen the relief attained by these release techniques.
A more aggressive pharmaceutical option is an injection of cortisone, to reduce swelling and nerve pressure within the carpal tunnel.
Methylcobalamin (vitamin B12) has been helpful in some cases of CTS.
There are several carpal tunnel release surgery variations: each surgeon has differences of preference based on their personal beliefs and experience. All techniques have several things in common, involving brief outpatient procedures; palm or wrist incision(s); and cutting of the transverse carpal ligament.
The two major types of surgery are open carpal tunnel release and endoscopic carpal tunnel release. Most surgeons historically have performed the open procedure, widely considered to be the gold standard. However, a growing number of surgeons now are offering endoscopic carpal tunnel release, which has been available since the 1990s. Open surgery involves an incision somewhere on the palm about an inch or two in length. Through this incision the skin and subcutaneous tissue is divided followed by the palmar fascia and ultimately the transverse carpal ligament. Endoscopic techniques involve one or two smaller incisions (less than half inch each) through which instrumentation is introduced including a synovial elevator, probes, knives and an endoscope used to fully visualize the underside of the transverse carpal ligament. The endoscopic methods do not divide the subcutaneous tissues or the palmar fascia to the same degree as the open method does.
Many studies have been done to determine whether the perceived benefits of a limited endoscopic or arthroscopic release are truly significant. Brown et al. did prospective, randomized, multi-center study and found no significant differences between the two groups with regard to the secondary quantitative outcome measurements. However the open technique resulted in more tenderness of the scar than did the endoscopic method. A prospective randomized study done in 2002 by Trumble revealed that good clinical outcomes and patient satisfaction are achieved more quickly when the endoscopic method of carpal tunnel release is used. Single-portal endoscopic surgery is a safe and effective method of treating carpal tunnel syndrome. There was no significant difference in the rate of complications or the cost of surgery between the two groups. However the open technique resulted in greater scar tenderness during the first three months after surgery as well as a longer time until the patients could return to work. http://www.ejbjs.org/cgi/content/abstract/84/7/1107
Some surgeons have suggested that in their own hands endoscopic carpal tunnel release has been associated with a higher incidence of median nerve injury, and for this reason it has been abandoned at several centers in the United States. For example, at the 2007 annual meeting of the American Society for Surgery of the Hand, during the "Journal of Retraction" event, one former advocate of endoscopic carpal tunnel release, Thomas J. Fischer, MD, publicly retracted his advocacy of the technique, based on his assessment that the benefit of the procedure (slightly faster recovery) did not outweigh the risk of injury to the median nerve. Despite these views many other surgeons have embraced limited incision methods and it is considered to be the procedure of choice for many of these surgeons with respect to idiopathic carpal tunnel syndrome. Supporting this are the results of some of the previously mentioned series which cite no difference in the rate of complications for either method of surgery. Thus there has been broad support for either surgical procedure: open or endoscopic carpal tunnel release using a variety of devices or incisions with the knowledge that the primary goal of any carpal tunnel release surgery is to divide the transverse carpal ligament and the distal aspect of the volar ante brachial fascia thereby decompressing the median nerve. http://orthoinfo.aaos.org/topic.cfm?topic=A00005
All of the surgical options (when performed without complication) typically have relatively rapid recovery profiles (weeks to a few months depending on the activity and technique), and all usually leave a cosmetically acceptable scar.
Carpal tunnel surgery is usually performed by a hand surgeon, orthopaedic or plastic surgeon; some neurosurgeons and general surgeons also perform the procedure.
While outcomes are generally good, certain factors can contribute to poorer results that have little to do with nerves, anatomy, or surgery type. One study showed that mental status parameters, alcohol use, yield much poorer overall results of treatment.
Many mild carpal tunnel syndrome sufferers either change their hand use, pattern, or posture at work or find a conservative, non-surgical treatment that allows them to return to full activity without hand numbness or pain, and without sleep disruption. Some find relief by adjusting their repetitive movements, the frequency with which they do the movements, and the amount of time they rest between periods of performing the movements. Other people end up prioritizing their activities and possibly avoiding certain hand activities so that they can minimize pain and perform the essential tasks. Keyboard re-mapping software can help people whose condition is aggravated by one-handed key strokes involving a combination of the Control, Shift, or Alt keys and an alpha-numeric key. Programs such as Autohotkey allow a person to disable key combinations while they train themselves to use two hands to perform the offending key strokes.
Recurrence of carpal tunnel syndrome after successful surgery is rare. If a person has hand pain after surgery, it is most likely not due to carpal tunnel syndrome. It may be the case that a person who has hand pain after carpal tunnel release was diagnosed incorrectly, such that the carpal tunnel release has had no positive effect upon the patient's symptoms.
This article is licensed under the Creative Commons Attribution-ShareAlike License. It uses material from the Wikipedia article on "Carpal Tunnel Syndrome" All material adapted used from Wikipedia is available under the terms of the Creative Commons Attribution-ShareAlike License. Wikipedia® itself is a registered trademark of the Wikimedia Foundation, Inc.
The definitive treatment for carpal tunnel syndrome is carpal tunnel release surgery. This is effective at relieving symptoms and preventing further nerve damage, but established nerve dysfunction in the form of static (constant) numbness, atrophy, or weakness are usually permanent.
Most cases of CTS are idiopathic (without a specific cause). Some patients are genetically predisposed to develop the condition.
The diagnosis of CTS is often misapplied to patients who have activity-related arm pain, such as RSI.
Carpal Tunnel Syndrome History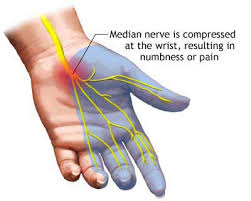
Although the condition was first noted in medical literature in the early 20th century, the first use of the term “carpal tunnel syndrome” was in 1939. The pathology was identified by physician Dr. George S. Phalen of the Cleveland Clinic after working with a group of patients in the 1950s and 1960s.Carpal Tunnel Syndrome Anatomy
The median nerve passes through the carpal tunnel, a canal in the wrist that is surrounded by bone on three sides, and a transverse carpal ligament on the fourth. Nine tendons—the flexor tendons of the hand—pass through this canal. The median nerve can be compressed by a decrease in the size of the canal, an increase in the size of the contents (such as the swelling of lubrication tissue around the flexor tendons), or both. Simply flexing the wrist to 90 degrees will decrease the size of the canal.Compression of the median nerve as it runs deep to the transverse carpal ligament (TCL) causes wasting of the thenar eminence, weakness of the flexor pollicis brevis, opponens pollicis, abductor pollicis brevis, as well as sensory loss in the distribution of the median nerve distal to the transverse carpal ligament. There is a superficial sensory branch of the median nerve, which branches proximal to the TCL and travels superficial to it. This branch is therefore spared, and it innervates the palm towards the thumb.
Carpal Tunnel Syndrome Symptoms
Many people who have carpal tunnel syndrome have gradually increasing symptoms over time. The first symptoms of CTS may appear when sleeping and typically include numbness and paresthesia (a burning and tingling sensation) in the thumb, index, and middle fingers, although some patients may experience symptoms in the palm as well. CTS is sometimes associated with trauma, pregnancy,multiple myeloma, amyloidosis, rheumatoid arthritis, acromegaly, mucopolysaccharidoses, orhypothyroidism.Genetic
The most important risk factors for carpal tunnel syndrome are structural and biological rather than environmental or activity-related. The strongest risk factor is genetic predisposition.
Work related
The international debate regarding the relationship between CTS and repetitive motion in work is ongoing. The Occupational Safety and Health Administration (OSHA) has adopted rules and regulations regarding cumulative trauma disorders. Occupational risk factors of repetitive tasks, force, posture, and vibration have been cited. However, the American Society for Surgery of the Hand (ASSH) has issued a statement that the current literature does not support a causal relationship between specific work activities and the development of diseases such as CTS.The relationship between work and CTS is controversial; in many locations workers diagnosed with carpal tunnel syndrome are entitled to time off and compensation. Carpal tunnel syndrome results in billions of dollars of workers compensation claims every year.
Some speculate that carpal tunnel syndrome is provoked by repetitive grasping and manipulating activities and that the exposure can be cumulative. It has also been stated that symptoms are commonly exacerbated by forceful and repetitive use of the hand and wrists in industrial occupations, but it is unclear if this refers to pain (which may not be due to carpal tunnel syndrome) or the more typical numbness symptoms.
A review of available scientific data by the National Institute for Occupational Safety and Health (NIOSH) indicated that job tasks that involve highly repetitive manual acts or specific wrist postures were associated with incidents of CTS, but causation was not established, and the distinction from work related arm pains that are not carpal tunnel syndrome was not clear. It has been proposed that repetitive use of the arm can affect the biomechanics of the upper limb or cause damage to tissues. It has also been proposed that postural and spinal assessment along with ergonomic assessments should be included in the overall determination of the condition. While addressing these factors has been found to improve comfort in some studies, there is no evidence that they affect the natural history of carpal tunnel syndrome.
Psychosocial factors
Studies have related activity-related upper extremity pain with psychological and social factors, but most such pains are nonspecific but commonly mislabeled as carpal tunnel syndrome. Psychological distress correlates with increased pain at work, as do other psychosocial stressors such as job demands, poor support from colleagues, and work dissatisfaction.As mentioned elsewhere on this page, carpal tunnel is characterized by numbness, not pain. Therefore, any associations between stress and carpal tunnel syndrome are debatable.
Trauma related
- Fractures of one of the arm bones, particularly a Colles' fracture.
- Dislocation of one of the carpal bones.
- Strong blunt trauma to the wrist or lower forearm, incurred for example by using arm extremity to cushion a fall or protecting oneself from falling heavy objects.
- Internal hemorrhaging at the wrist.
- Deformities from abnormal healing of old bone fractures.
- Electrical burns may cause acute carpal tunnel syndrome.
Carpal tunnel syndrome associated with other diseases
Non-traumatic causes generally happen over a period of time, and are not triggered by one certain event. Many of these factors are manifestations of physiologic aging.Examples include:
- Rheumatoid arthritis and other diseases that cause inflammation of the flexor tendons.
- With pregnancy and hypothyroidism, fluid is retained in tissues, which swells the tenosynovium.
- Acromegaly, a disorder of growth hormones, compresses the nerve by the abnormal growth of bones around the hand and wrist.
- Tumors (usually benign), such as a ganglion or a lipoma, can protrude into the carpal tunnel, reducing the amount of space. This is exceedingly rare (less than 1%).
- Obesity also increases the risk of CTS: individuals who are classified as obese (BMI > 29) are 2.5 times more likely than slender individuals (BMI < 20) to be diagnosed with CTS.
- ''Double crush syndrome'' is a speculative and debated theory which postulates that when there is compression or irritation of nerve branches contributing to the median nerve in the neck or anywhere above the wrist, this then increases the sensitivity of the nerve to compression in the wrist. There is little evidence, however, that this syndrome really exists.
Carpal Tunnel Syndrome Diagnosis
The reference standard for the diagnosis of carpal tunnel syndrome is electrophysiological testing. Patients with intermittent numbness in the distribution of the median nerve and positive Phalen's and Durkan's tests, but normal electrophysiological testing have—at worst—very mild carpal tunnel syndrome. A predominance of pain rather than numbness is unlikely to be due to carpal tunnel syndrome no matter the result of electrophysiological testing.Clinical assessment by history taking and physical examination can support a diagnosis of CTS.
- Phalen's maneuver is performed by flexing the wrist gently as far as possible, then holding this position and awaiting symptoms. A positive test is one that results in numbness in the median nerve distribution when holding the wrist in acute flexion position within 60 seconds. The quicker the numbness starts, the more advanced the condition.
- Tinel's sign, a classic, though less specific test, is a way to detect irritated nerves. Tinel's is performed by lightly tapping the skin over the flexor retinaculum to elicit a sensation of tingling or "pins and needles" in the nerve distribution.
- Durkan test, ''carpal compression test'', or applying firm pressure to the palm over the nerve for up to 30 seconds to elicit symptoms has also been proposed.
The role of MRI or ultrasound imaging in the diagnosis of carpal tunnel syndrome is unclear.
Carpal Tunnel Syndrome Prevention
Some think that the current best evidence suggests that carpal tunnel syndrome is an inherent, structural disease determined primarily by one's genes.Recommendations for preventing carpal tunnel syndrome have poor scientific support. Current recommendations generally don't suggest immobilizing braces, but instead activity modification and non-steroidal anti-inflammatory drugs as initial therapy, followed by more aggressive options or specialist referral if symptoms do not improve.
Many health professionals suggest that, for best results, one should wear braces at night and, if possible, during the activity primarily causing stress on the wrists.
Localized steroid injections
Steroid injections can be quite effective for temporary relief from symptoms of CTS for a short time frame while a patient develops a longterm strategy that fits with his/her lifestyle. In certain patients, an injection may also be of diagnostic value. This treatment is not appropriate for extended periods, however. In general, medical professionals only prescribe local steroid injections until other treatment options can be identified. For most patients, surgery is the only option that will provide permanent relief.
Physiotherapy
There is little evidence to support the use of physiotherapy or occupational therapy techniques for carpal tunnel syndrome. They seem to be oriented primarily towards non-specific activity related pain rather than the numbness of carpal tunnel syndrome. The following comments regarding physical therapy seem to apply more to such chronic activity related pains than to verifiable idiopathic median nerve compression at the carpal tunnel.Physiotherapy offers several ways to treat and control carpal tunnel syndrome. This procedure should be directed specifically towards the pattern of pain / symptoms and dysfunction assessed by the therapist. As such, it may include a range of modalities ranging from soft tissue massage, conservative stretches and exercises and techniques to directly mobilize the nerve tissue. It can also include the aforementioned immobilizing braces.
Clinically, sometimes a patient will present with a hand that is very inflamed and swollen with severe symptoms of pain, tingling and numbness and almost a fear of use because of the pain. In these cases a physiotherapist may focus on techniques to reduce the pain and inflammation, and exercises to encourage improved circulation. A comprehensive review of effectiveness of hand therapies in carpal tunnel management demonstrates that there is some valid scientific evidence for a range of therapeutic modalities.
For instance, Body Awareness Therapy such as the Feldenkrais method has positive effects in relation to fibromyalgia and chronic pain. Structured exercise programs using these therapies to reduce wrist pain have been developed.
Occupational therapy
The comments provided in this section appear more suited to nonspecific activity related arm pains that to true carpal tunnel syndrome (verifiable idiopathic median nerve compression at the carpal tunnel).Occupational therapy offers ergonomic suggestions to prevent worsening of the symptoms and occupational therapist facilitates hand functions through functional activities and helps to regain the functions which are necessary for the functional living through remedial adaptive approaches.
Any forceful and repetitive use of the hands and wrists can cause upper extremity pain. More frequent rest can be useful if it can be orchestrated into one's schedule. It has been shown that taking multiple mini breaks during the stressful activity is more effective than taking occasional long breaks. There are computer applications that aid users in taking breaks. All of these applications have recommended defaults, following the most effective average break configuration, which is a 30 sec. pause every 3 to 5 minutes (the more severe the pain, the more often one should take this break). There are also programs that automatically click the mouse. Before investing in these types of programs, it's best to consult with a doctor and research whether computer use is causing or contributing to the symptoms, as well as getting a formal diagnosis.
More pro-active ways to reducing the stress on the wrists which will alleviate wrist pain and strain involve adopting a more ergonomic work and life environment. Switching from a QWERTY computer keyboard layout to a more optimised ergonomic layout such as Dvorak was commonly cited as beneficial in early CTS studies, however some meta-analyses of these studies claim that the evidence that they present is limited.
It is also important that one's body be aligned properly with the keyboard. This is most easily accomplished by bending ones elbows to a 90 degree angle and making sure the keyboard is at the same height as the elbows. Also it is important not to put physical stress on the wrists by hanging the wrist on the edge of a desk, or exposing the wrists to strong vibrations (e.g. manual lawn mowing). Position the computer monitor directly in front of your seat, so the neck is not twisted to either side when viewing the screen.
Exercises that relax and strengthen the muscles of the upper back can reduce the risk of a ''double crush'' of the median nerve.
Massage is one of the most overlooked methods for treatment of the symptoms of CTS. The use of myofascial release and active stretch release can erase the pain, numbness, tingling and burning in minutes. Then following up with the stretches and exercises afore mentioned will lengthen the relief attained by these release techniques.
Medication
Using an over-the-counter anti-inflammatory such as aspirin, ibuprofen or naproxen can be effective as well for controlling symptoms. Pain relievers like paracetamol will only mask the pain, and only an anti-inflammatory will affect inflammation. Non-steroidal anti-inflammatory medications theoretically can treat the swelling and thus the source of the problem. Oral steroids such as prednisone do the same, but are generally not used for this purpose because of significant side effects. Use of non-steroidal anti-inflammatory drugs may worsen asthma symptoms in some with a history of asthma, making the use of steroids such as prednisone the safer option for treating CTS. The most common complications associated with long-term use of anti-inflammatory medications are gastrointestinal irritation and bleeding. Also, some anti-inflammatory medications have been linked to heart complications. Use of anti-inflammatory medication for chronic, long-term pain should be done with doctor supervision.A more aggressive pharmaceutical option is an injection of cortisone, to reduce swelling and nerve pressure within the carpal tunnel.
Methylcobalamin (vitamin B12) has been helpful in some cases of CTS.
Carpal tunnel release surgery
Release of the transverse carpal ligament is known as "carpal tunnel release" surgery. It is recommended when there is static (constant, not just intermittent) numbness, muscle weakness, or atrophy, and when night-splinting no longer controls intermittent symptoms. In general, milder cases can be controlled for months to years, but severe cases are unrelenting symptomatically and are likely to result in surgical treatment.Procedure
In carpal tunnel release surgery, the goal is to divide the transverse carpal ligament in two. This is a wide ligament that runs across the hand, from the scaphoid bone to the hamate bone and pisiform. It forms the roof of the carpal tunnel, and when the surgeon cuts across it (i.e., in a line with the ring finger) it no longer presses down on the nerve inside, relieving the pressure.There are several carpal tunnel release surgery variations: each surgeon has differences of preference based on their personal beliefs and experience. All techniques have several things in common, involving brief outpatient procedures; palm or wrist incision(s); and cutting of the transverse carpal ligament.
The two major types of surgery are open carpal tunnel release and endoscopic carpal tunnel release. Most surgeons historically have performed the open procedure, widely considered to be the gold standard. However, a growing number of surgeons now are offering endoscopic carpal tunnel release, which has been available since the 1990s. Open surgery involves an incision somewhere on the palm about an inch or two in length. Through this incision the skin and subcutaneous tissue is divided followed by the palmar fascia and ultimately the transverse carpal ligament. Endoscopic techniques involve one or two smaller incisions (less than half inch each) through which instrumentation is introduced including a synovial elevator, probes, knives and an endoscope used to fully visualize the underside of the transverse carpal ligament. The endoscopic methods do not divide the subcutaneous tissues or the palmar fascia to the same degree as the open method does.
Many studies have been done to determine whether the perceived benefits of a limited endoscopic or arthroscopic release are truly significant. Brown et al. did prospective, randomized, multi-center study and found no significant differences between the two groups with regard to the secondary quantitative outcome measurements. However the open technique resulted in more tenderness of the scar than did the endoscopic method. A prospective randomized study done in 2002 by Trumble revealed that good clinical outcomes and patient satisfaction are achieved more quickly when the endoscopic method of carpal tunnel release is used. Single-portal endoscopic surgery is a safe and effective method of treating carpal tunnel syndrome. There was no significant difference in the rate of complications or the cost of surgery between the two groups. However the open technique resulted in greater scar tenderness during the first three months after surgery as well as a longer time until the patients could return to work. http://www.ejbjs.org/cgi/content/abstract/84/7/1107
Some surgeons have suggested that in their own hands endoscopic carpal tunnel release has been associated with a higher incidence of median nerve injury, and for this reason it has been abandoned at several centers in the United States. For example, at the 2007 annual meeting of the American Society for Surgery of the Hand, during the "Journal of Retraction" event, one former advocate of endoscopic carpal tunnel release, Thomas J. Fischer, MD, publicly retracted his advocacy of the technique, based on his assessment that the benefit of the procedure (slightly faster recovery) did not outweigh the risk of injury to the median nerve. Despite these views many other surgeons have embraced limited incision methods and it is considered to be the procedure of choice for many of these surgeons with respect to idiopathic carpal tunnel syndrome. Supporting this are the results of some of the previously mentioned series which cite no difference in the rate of complications for either method of surgery. Thus there has been broad support for either surgical procedure: open or endoscopic carpal tunnel release using a variety of devices or incisions with the knowledge that the primary goal of any carpal tunnel release surgery is to divide the transverse carpal ligament and the distal aspect of the volar ante brachial fascia thereby decompressing the median nerve. http://orthoinfo.aaos.org/topic.cfm?topic=A00005
All of the surgical options (when performed without complication) typically have relatively rapid recovery profiles (weeks to a few months depending on the activity and technique), and all usually leave a cosmetically acceptable scar.
Efficacy
Surgery to correct carpal tunnel syndrome has a high success rate. Up to 90% of patients were able to return to their same jobs after surgery. In general, endoscopic techniques are as effective as traditional open carpal surgeries, though the faster recovery time typically noted in endoscopic procedures is felt by some to possibly be offset by higher complication rates. Success is greatest in patients with the most typical symptoms. The most common cause of failure is incorrect diagnosis, and it should be noted that this surgery will only mitigate carpal tunnel syndrome, and will not relieve symptoms with alternative causes. Recurrence is rare, and apparent recurrence usually results from a misdiagnosis of another problem. Complications can occur, but serious ones are infrequent to rare.Carpal tunnel surgery is usually performed by a hand surgeon, orthopaedic or plastic surgeon; some neurosurgeons and general surgeons also perform the procedure.
Carpal Tunnel Syndrome Long Term Recovery
Most people who find relief of their carpal tunnel symptoms with conservative or surgical management find minimal residual or "nerve damage". Long-term chronic carpal tunnel syndrome (typically seen in the elderly) can result in permanent "nerve damage", i.e. irreversible numbness, muscle wasting and weakness.While outcomes are generally good, certain factors can contribute to poorer results that have little to do with nerves, anatomy, or surgery type. One study showed that mental status parameters, alcohol use, yield much poorer overall results of treatment.
Many mild carpal tunnel syndrome sufferers either change their hand use, pattern, or posture at work or find a conservative, non-surgical treatment that allows them to return to full activity without hand numbness or pain, and without sleep disruption. Some find relief by adjusting their repetitive movements, the frequency with which they do the movements, and the amount of time they rest between periods of performing the movements. Other people end up prioritizing their activities and possibly avoiding certain hand activities so that they can minimize pain and perform the essential tasks. Keyboard re-mapping software can help people whose condition is aggravated by one-handed key strokes involving a combination of the Control, Shift, or Alt keys and an alpha-numeric key. Programs such as Autohotkey allow a person to disable key combinations while they train themselves to use two hands to perform the offending key strokes.
Recurrence of carpal tunnel syndrome after successful surgery is rare. If a person has hand pain after surgery, it is most likely not due to carpal tunnel syndrome. It may be the case that a person who has hand pain after carpal tunnel release was diagnosed incorrectly, such that the carpal tunnel release has had no positive effect upon the patient's symptoms.
This article is licensed under the Creative Commons Attribution-ShareAlike License. It uses material from the Wikipedia article on "Carpal Tunnel Syndrome" All material adapted used from Wikipedia is available under the terms of the Creative Commons Attribution-ShareAlike License. Wikipedia® itself is a registered trademark of the Wikimedia Foundation, Inc.

No comments:
Post a Comment